Is Healthcare AI Shifting from Pilots to Practice?
Healthcare's latest AI announcements focused on deployment, not experimentation or future promises.
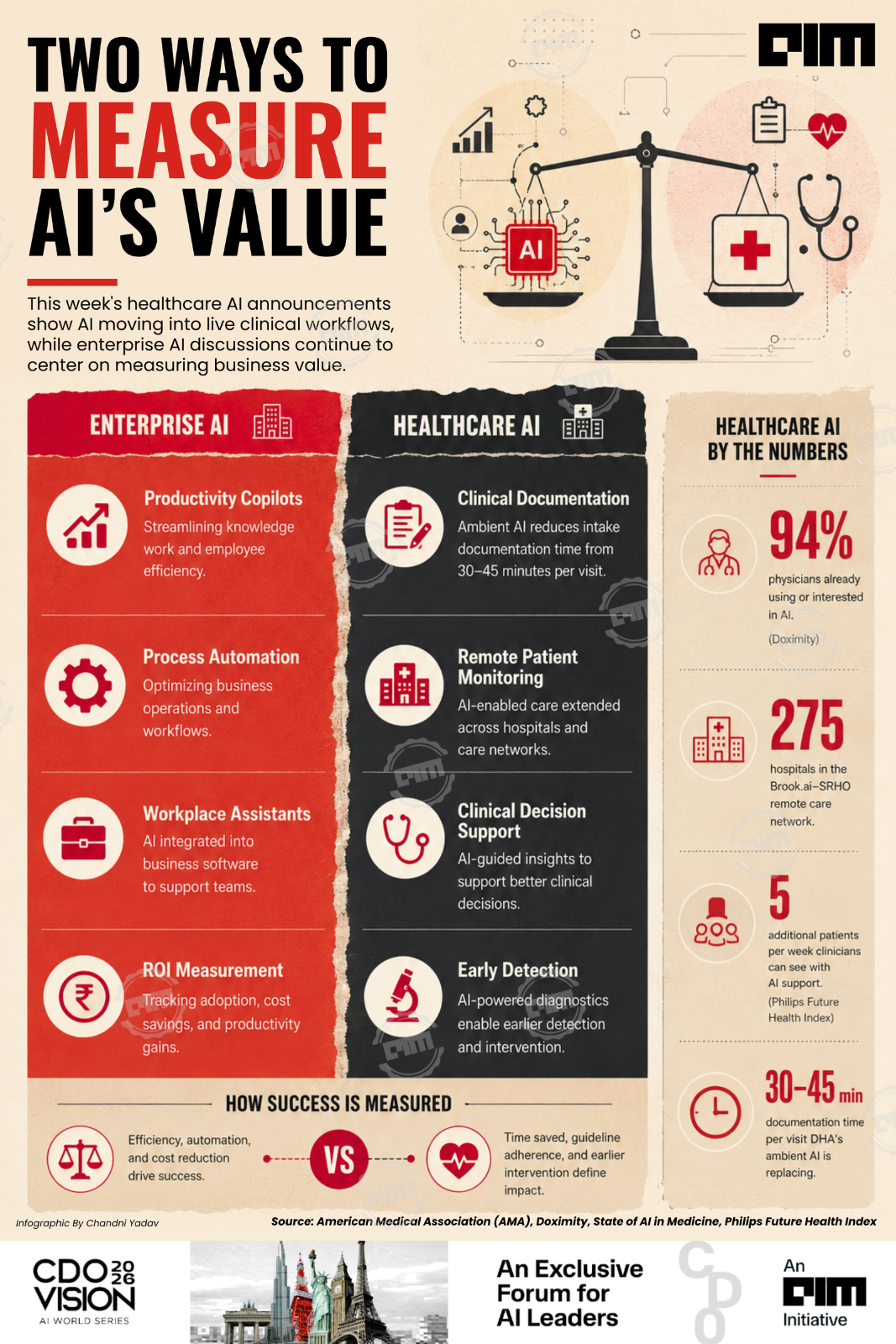
While enterprise AI spent another week debating governance frameworks, inference costs, and return on investment, healthcare organizations announced AI deployments across nearly every stage of clinical care.
Healthcare and life sciences organizations spent the same week announcing AI deployed directly into clinical workflows. Several stories from the past few days show AI already moving through documentation, remote monitoring, physician decision-making, and diagnostics in daily clinical use.
Healthcare is not the largest AI adopter by every measure, but it is increasingly where AI is moving beyond pilots into routine clinical practice.
Last week's announcements span the care pathway
Documentation is the burden clinicians describe most often. The Defense Health Agency announced a completed global rollout of its ambient-listening Clinical AI Agent, which records patient visits with consent and turns them into structured notes.
At Wilford Hall, Col. Stephen Edstrom said his intake documentation used to take 30 to 45 minutes per visit before ambient listening took over.
Care is also extending past hospital walls. SRHO and Brook.ai partnered to expand AI-enabled remote monitoring across 275 hospitals, bringing clinical oversight into patients' homes.
Inside the hospital, AI is reaching earlier into the decision itself. OpenEvidence and the Anticoagulation Forum announced a partnership putting AI-guided evidence directly into anticoagulation decisions, among the highest-stakes, most probability-driven calls in medicine.
Geoff Barnes, MD, president of the AC Forum, called antithrombotic therapy one of the most effective, and also one of the highest-risk areas in medicine, since clinicians must weigh clot prevention against bleeding risk in real time.
OpenEvidence's Chief Medical Officer, Travis Zack, said clinicians are increasingly turning to AI to navigate the growing complexity of medical evidence.
Diagnosis is moving earlier in the pathway too. Caris Life Sciences launched an AI-powered blood test for early multi-cancer detection.
 >
>Taken together, last week's stories touched documentation, remote care, decision support, and diagnostics: most of the clinical pathway, inside a single week, and likely an undercount of everything that shipped.
Why medicine is a better fit for this moment
Healthcare is moving faster than the enterprise debate suggests, for a few reasons.
AI solves an acute, immediate workforce problem in burnout and documentation burden, where saving even 20 to 30 minutes a day has obvious operational value.
Medicine also runs on the things AI is good at: probability, guidelines, pattern recognition. Decision support tools like OpenEvidence's plug directly into that process, surfacing evidence at the moment a clinician needs it.
The infrastructure bets point the same direction. Mayo Clinic and Microsoftannounced a collaboration to build a frontier AI model trained on Mayo's own clinical data. Mayo will own the model, treating clinical AI as core infrastructure it builds and keeps in-house.
Healthcare also measures success in terms it already tracks. Philips' 2026 Future Health Index found clinicians seeing a median of five additional patients per week using AI, with 27% saying AI helped catch possible medical errors multiple times in three months.
AMA's 2026 survey found more than 80% of physicians now use AI professionally, roughly double the 2023 rate.
Governance is catching up to adoption
Enterprise AI is still debating whether the investment pays off. In healthcare, that argument looks largely settled, with clinicians using these tools daily and this week's stories showing AI built into standard practice.
What healthcare is now building is the layer underneath that adoption. CMS recently stood up a new Office of Health Technology Products to oversee AI and interoperability. The WHO has separately urged policymakers to keep automated systems in a supporting role, with human judgment retaining final say in health policy.
Training lags behind use. 77% of clinicians in Philips' survey still call their AI training inadequate or inconsistent.
The conversation has moved from whether AI belongs in medicine to how it should be overseen. That's a sign clinical AI has become normal, even as the harder work on trust and validation remains ahead.
Enterprise AI is still building its business case. Medicine is already running the experiment in production, one hospital system and one workflow at a time.
Key Takeaways
- Highlight AI's shift from experimentation to deployment in healthcare across clinical workflows.
- Emphasize the global rollout of ambient-listening AI agents for efficient documentation.
- Showcase partnerships expanding AI-enabled remote monitoring into patients' homes.
- Note AI's role in enhancing clinical decision-making within hospitals.
- Recognize healthcare's growing adoption of AI beyond pilot projects to routine practice.